This 73 year old healthy woman saw her gynecologist for a routine evaluation and mentioned that she had increasing urinary frequency including nocturia. She is a former smoker with a 30 pack/year history. She has not had major surgery.
A urinalysis indicated microscopic hematuria so the uro- gynecologist performed an office cystoscopy and saw a large bladder tumor. She was referred for consultation.
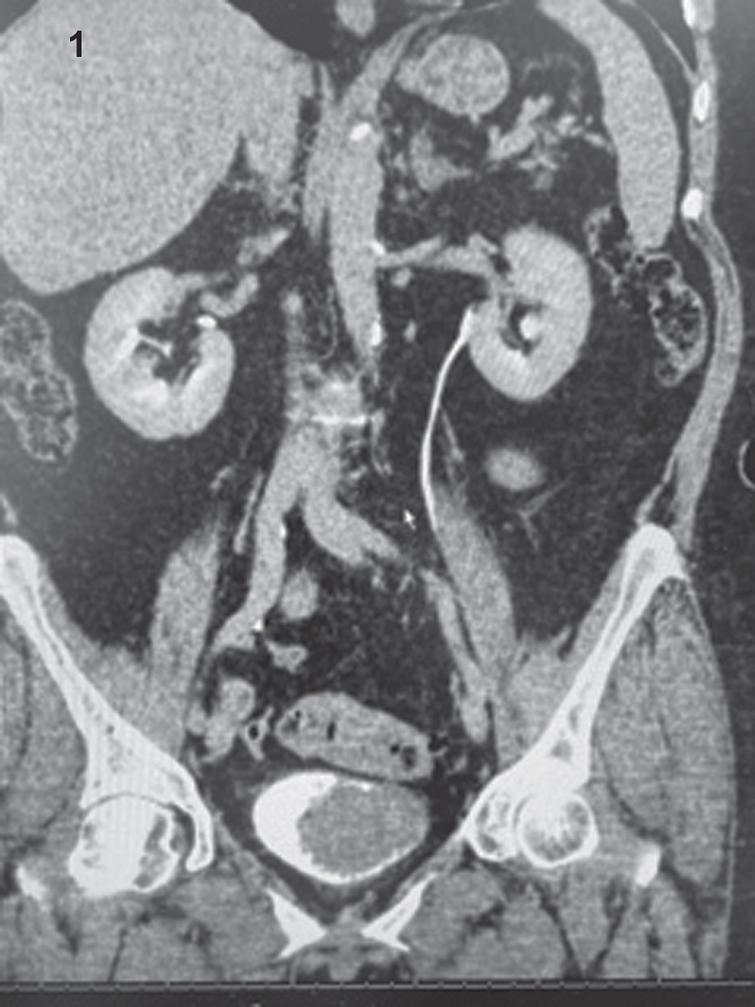
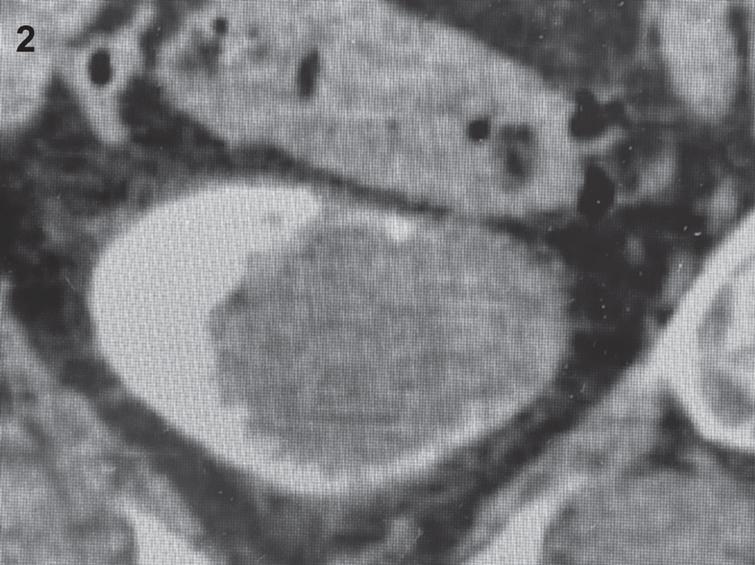
A CT scan indicated normal kidneys. There is no hydronephrosis. The left side of the bladder had a large filling defect consistent with bladder cancer. She did not have gross hematuria so the bladder mass was not related to blood clots.
As part of my initial examination I performed a cystoscopy in the office and, as expected, the entire left side of the bladder was occupied by papillary bladder cancer which appeared to be low grade.
The dilemma was how to proceed with pathologic diagnosis, staging, and removal of the tumor. The choices might be: 1. Resect as much tumor as possible with transurethral resection and reevaluate based on the pathology and success of removing the tumor endoscopically, 2. Perform a radical cystectomy since even if this is a Ta or T1 tumor the risk of “recurrence” is high and the chance of removing all of the tumor endoscopically is low, 3. Perform a cystotomy and remove the tumor while minimizing tumor “spillage.
I discussed the case with two experienced urologic oncology colleagues to whom I had sent the CT images. They both thought a cystectomy would be best.
Figs. 1–3
CT images demonstrating large filling defect in the bladder.
Figs. 4–7
Endoscopic views of the large papillary bladder tumor.
I proceeded with a TUR BT. The first session lasted 3 hours and about 50% of the tumor was removed. The patient was placed on CBI. The next day the irrigation was not clear with the CBI off and thus I could not discharge her, wait for the pathology report and proceed with either another TUR BT or a cystectomy depending on the grade and stage. She was returned to the operating room and after another one hour transurethral resection all of the visible tumor was removed. The pathology was high grade Ta. Muscle was present and uninvolved.
As we often say “all TUR BTs are not the same”. The vast majority of patients present with either small or medium sized papillary Ta tumor(s) or an obvious muscle invasive bladder cancer. The TUR BT for the first category is usually quite straightforward although the location of the tumor or the patient’s anatomy might be a challenge. In the patient with an apparent MIBC, the first priority is to document the extent of invasion and secondly to perform a “complete” resection without perforating the bladder or causing significant hematuria. The case presented here requires judgement and endurance. One wants to attempt a complete resection without excessive damage to the bladder or bleeding.
INFORMED CONSENT
Written informed consent for publication was obtained from the patient.
ETHICAL CONSIDERATIONS
The author has institutional review board approval for reviewing bladder cancer cases for outcome (MHS.2020.026).
CONFLICT OF INTEREST
Nothing to disclose.

