RF is a 73 year old man with his first episode of bladder cancer. He underwent a renal transplant in 2005 and his current creatinine is 1.20. His performance status is quite reasonable. He was a heavy cigarette smoker with a 30 pack/year history and stopped smoking at age 50.
He has a pacemaker. He recently underwent a right carotid endarterectomy.
He had gross hematuria in 11/18. A CT scan revealed 2 small native kidneys and a functioning transplant kidney in the right pelvis. There were filling defects in the urinary bladder. There were no enlarged pelvic lymph nodes.
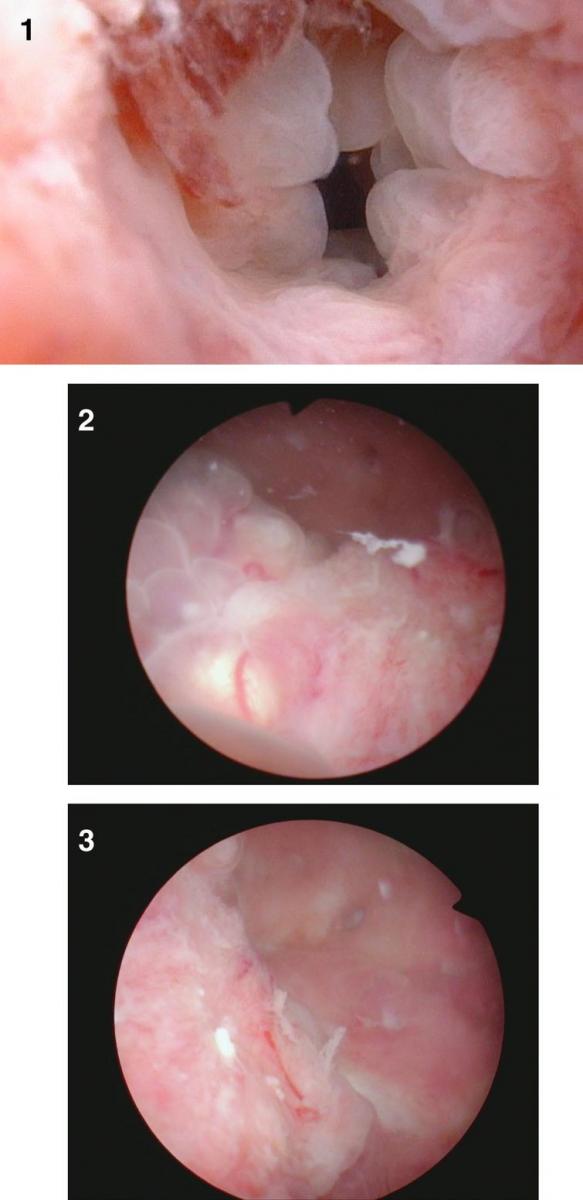
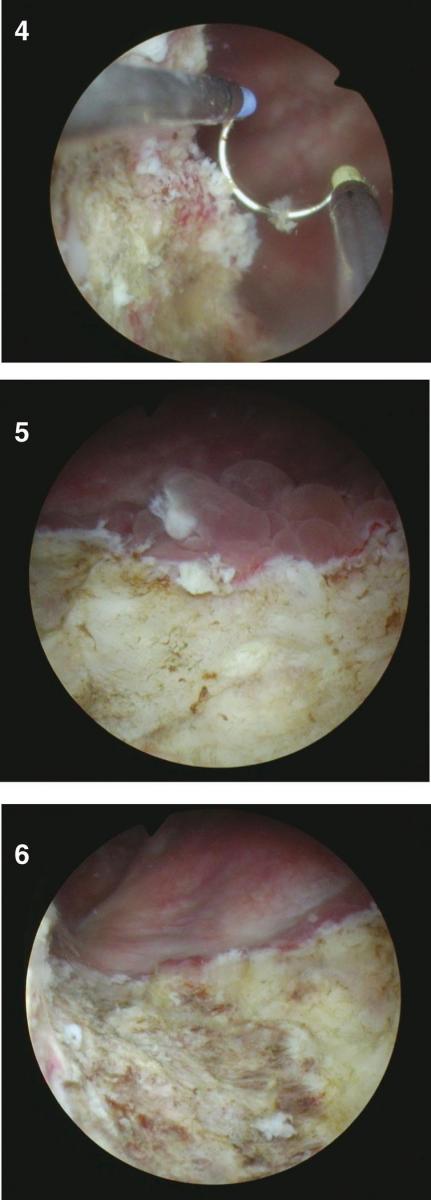
Cystoscopic examination indicated extensive urothelial cancer of the bladder with extension of the tumor into the prostatic urethra (Figs. 1–3). An extensive transurethral resection was performed and much of the tumor was resected (Figs. 4–6). A bimanual examination indicated that the bladder and prostate were mobile, cT3.
Figs.1–3
Sessile tumor in the bladder and extending to the bladder neck and into the prostatic urethra.
Figs.4–6
Tumor resection.
The pathology revealed not surprisingly a high grade urothelial carcinoma which invaded deep into the muscualris propria and extended into the proximal prostatic urethra.
The next decision was whether to prescribe neoadjuvant chemotherapy. After considering his general medical status and the immunosuppression we elected to proceed with a radical cystoprostatectomy and ileal conduit urinary diversion. The pathology indicated that the tumor extended to the serosa of the bladder and involved the prostatic stroma. Two of 12 left pelvic lymph nodes contained metastatic cancer.
We invite our readers to review and comment on the case and management by using the online comment section below the case:
https://www.bladdercancerjournal.com/challenging-cases
CONFLICTS OF INTEREST
Nothing to disclose.

